
Minimally invasive skin incisions conceal extensive deep tissue damage after surgery.
Thermal injury from electrocoagulation, serosal damage induced by pneumoperitoneum and soft tissue traction trigger chronic low-grade inflammation, resulting in pathological retention and persistent contraction of myofibroblasts to form permanent tension anchor points.
Local tension propagates across the systemic fascial continuum toward the craniosacral system, disrupts autonomic homeostasis and proprioceptive input, and eventually causes systemic postural compensation. This article systematically elaborates the molecular, cellular and holistic mechanisms of this pathological process and proposes targeted intervention protocols based on craniosacral therapy.
• Characteristics of occult deep tissue injury after minimally invasive surgery
A common misconception equates minimally invasive surgery with minor surgery. Despite only 5–10 mm cutaneous incisions, intraoperative deep trauma features wide distribution, high concealment and long duration:
1. Electrocoagulation thermal injury: High temperature generated by monopolar electrocautery and ultrasonic scalpel creates a 3–5 mm thermal necrotic zone penetrating full fascial layers and visceral serosa. Slow resorption of necrotic tissue induces persistent chronic low-grade inflammation lasting 6 to 12 months.
2. Pneumoperitoneum-related injury: Constant intra-abdominal pressure of 12–15 mmHg during laparoscopy triggers widespread ischemic-hypoxic apoptosis of peritoneal mesothelial cells and destroys the peritoneal lubrication barrier. Inflammatory mediators released by damaged mesothelium diffuse throughout the peritoneal cavity and lay the foundation for extensive intra-abdominal adhesions.
3. Serosal barrier disruption: Surgical trauma destroys the simple epithelial structure of peritoneum, pleura and joint synovium and abolishes their physiological function of synovial secretion and anti-adhesion. Fibrin exudate on adjacent tissues cannot be fully degraded by fibrinolytic system and evolves into primary fibrin adhesions. Such lesions are undetectable via imaging and routine physical examination, yet abnormal tissue repair triggered by these injuries constitutes the primary cause of long-term postoperative complications.
• Pathological retention of myofibroblasts: Cytological basis of scar contracture
Wound healing proceeds as an orderly biological cascade; as key effector cells, myofibroblasts follow a physiological cycle of “activation – contraction – apoptosis – clearance”. Unique traumatic microenvironment after minimally invasive surgery enables myofibroblasts to acquire apoptosis-resistant phenotype and lodge permanently within tissues:
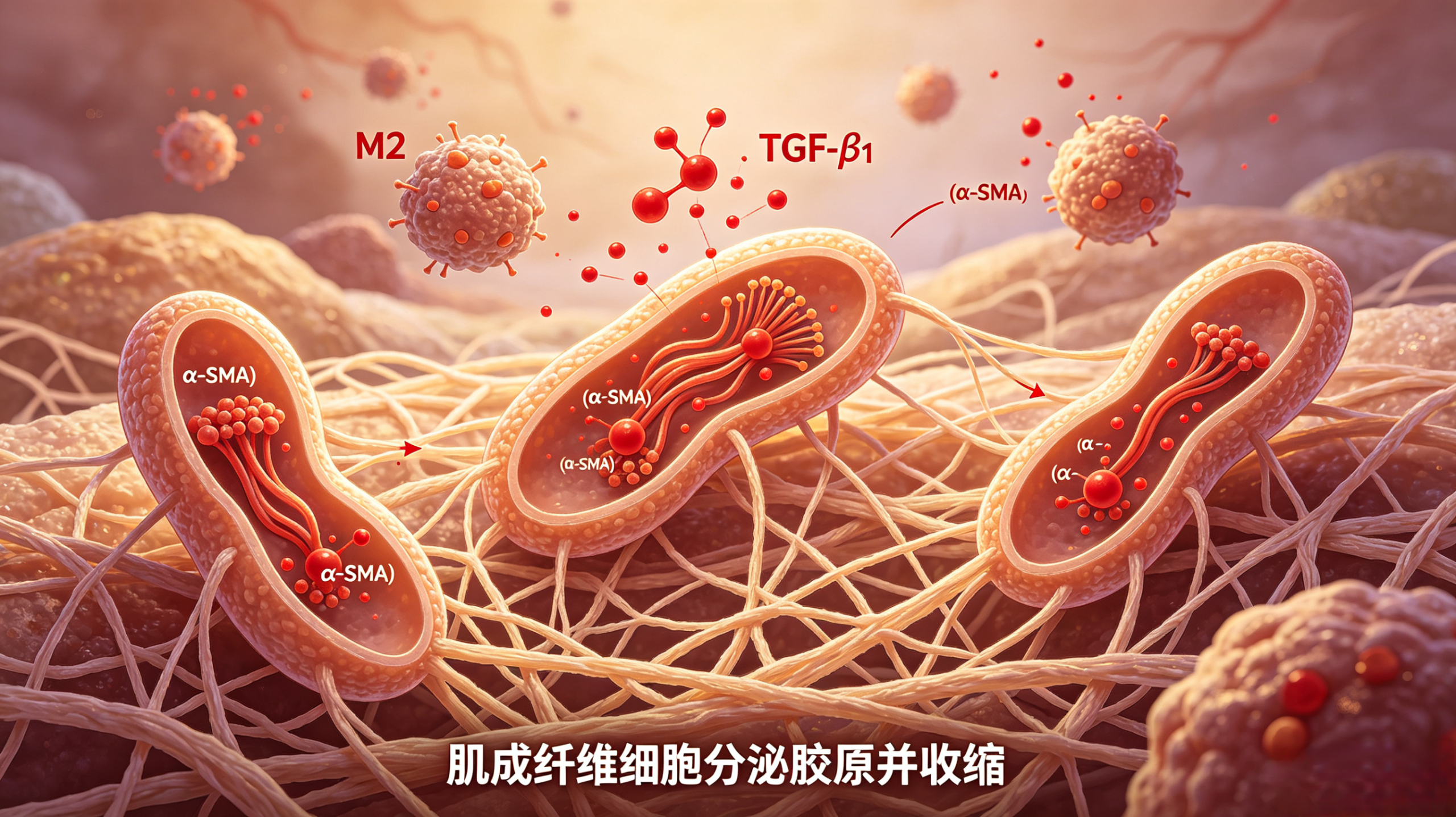
1. Biochemical-mediated apoptosis inhibition: Sustained chronic inflammation stimulates M2 macrophages to over-secrete transforming growth factor-β1 (TGF-β1). TGF-β1 activates PI3K/AKT pathway to upregulate anti-apoptotic proteins BCL-2, BCL-XL and XIAP, which directly inactivate effector caspase and block programmed cell death at molecular level.
2. Mechanical-driven survival feedback loop: Myofibroblast contraction leads to massive deposition and irregular cross-linking of type I collagen, drastically elevating local tissue Young’s modulus. Stiff extracellular matrix upregulates anti-apoptotic and profibrotic genes via integrin-YAP/TAZ mechanotransduction, forming a positive-feedback cycle: cell contraction → matrix stiffening → sustained cell survival.
3. Imbalanced extracellular matrix degradation: The ratio of tissue inhibitor of metalloproteinases (TIMPs) to matrix metalloproteinases (MMPs) shifts abnormally within pathological scar microenvironment and hinders collagen breakdown. Cross-linked rigid collagen scaffolds anchor myofibroblasts firmly and further prevent cellular detachment and apoptosis.
4. Immune evasion mechanism: Impaired phosphatidylserine externalization on myofibroblast membrane prevents macrophage recognition of apoptotic markers; meanwhile cells secrete soluble Fas to neutralize cytotoxic immune signals for immune concealment. Persistently retained myofibroblasts continuously generate contractile force to build permanent deep-tissue tension anchors, accounting for progressive postural deformities years after surgery.
• Profibrotic amplification via autonomic-immune axis
Fibrosis progression is regulated by multiple neural pathways, with overactive sympathetic nervous system as the core driver:
1. Direct sympathetic regulation: Nerve impulses from brainstem sympathetic nuclei travel down spinal sympathetic chains to injured sites. Norepinephrine (NE) released from sympathetic terminals binds β2-adrenoceptors on fibroblast membrane, upregulates α-SMA expression and accelerates fibroblast-myofibroblast differentiation.
2. Macrophage polarization modulation: NE drives macrophages toward profibrotic M2 phenotype; M2 macrophages abundantly secrete TGF-β1, PDGF and other cytokines to construct local profibrotic microenvironment.
3. Mechano-neural reflex loop: Scar contracture pulls fascia and dura mater to activate nociceptive C-fibers and Aδ-fibers. Aberrant afferent signals transmit to spinal dorsal horn and cerebral somatosensory cortex and induce central sensitization. Centrally mediated vagal suppression and excessive sympathetic discharge further exacerbate regional fibrosis.
4. Systemic effects of HPA axis: Postoperative anxiety, pain and sleep disturbance activate hypothalamic-pituitary-adrenal (HPA) axis; chronic hypercortisolemia accelerates fibroblast activation and collagen accumulation to aggravate hypertrophic scarring.
• Tension transmission mechanism of fascial continuum and craniosacral system
Human deep fascia forms an uninterrupted connective tissue network enveloping muscles, nerves, blood vessels and visceral organs, serving as biomechanical highway for tension propagation. Scar-derived tension spreads throughout the body along fascial chains and ultimately influences the craniosacral system:
1. Core transmission pathway:
Tension originating from focal scar contracture propagates sequentially to craniosacral axis: superficial fascia → myofascia → visceral serosal fascia → prevertebral fascia → dural sheath → intracranial dura mater.
2. Three categories of craniosacral dysfunction:
– Mechanical restriction: Persistent dural traction limits cranial suture mobility and sacral excursion, slowing and desynchronizing craniosacral rhythm (6–12 cycles per minute).
– Cerebrospinal fluid circulation disorder: Impaired CSF pulsation obstructs glymphatic drainage and accumulates metabolic waste to deteriorate autonomic dysfunction.
– Proprioceptive dysfunction: Continuous abnormal afferent signals from dura and scar proprioceptors remodel CNS body map and trigger pathological movement patterns.
• Postoperative compensatory tension transmission by surgical site
Surgical trauma at distinct anatomical locations leads to divergent tension pathways and characteristic postural disorders:
– Laparoscopic surgery: Adhesions predominantly form at abdominal trocar sites, transversalis fascia and peritoneum. Tension descends along abdominal fascia to pelvic diaphragm and sacrum and ascends via thoracolumbar fascia to lumbar dura, manifesting as anterior pelvic tilt, lumbar hyperlordosis and upper crossed syndrome.
– Thoracoscopic surgery: Primary adhesion sites include parietal pleura, intercostal muscles and mediastinal fascia; unilateral pleural contracture pulls tension along thoracic vertebrae to deep cervical fascia and skull base, resulting in thoracic scoliosis, uneven shoulder height and ipsilateral head tilt.
– Arthroscopic surgery: Joint capsule, synovium and periarticular ligaments are prone to adhesion; capsular shrinkage disturbs lower limb alignment and induces functional leg length discrepancy, pelvic obliquity and compensatory spinal scoliosis.
– Spinal endoscopic surgery: Epidural space, paraspinal muscles and ligamentum flavum develop postoperative scarring; epidural adhesions directly pull dura and compress the whole craniosacral axis, causing decreased lumbar lordosis, protective trunk anteflexion and intermittent claudication.
• Intervention protocols of craniosacral therapy
Conventional rehabilitation focuses on muscle strengthening and joint mobility improvement without targeting core pathology: fascial adhesion and craniosacral imbalance.
Craniosacral therapy applies gentle manual manipulation to target multiple pathological nodes:
1. Dural tension release: Gentle mobilization of occiput, sacrum and spine releases epidural-dural adhesions, restores physiological craniosacral rhythm and disconnects biomechanical linkage between peripheral scar and central nervous system.
2. Mechanical stress reduction: Visceral and deep fascial release softens scar matrix, blocks YAP/TAZ pro-survival mechanopathway and induces myofibroblast apoptosis.
3. Vagus nerve stimulation: Cranial base manipulation activates intracranial vagus nerve to initiate cholinergic anti-inflammatory pathway, inhibit M2 macrophage polarization and lower local TGF-β1 concentration.
4. Extracellular matrix remodeling: Low-amplitude cyclic mechanical stimulation upregulates MMPs and downregulates TIMPs to promote degradation and orderly rearrangement of disorganized collagen.
5. Proprioceptive recalibration: Correct abnormal afferent input to help CNS reconstruct accurate body schema and eliminate chronic compensatory muscular hypertonicity. Clinical observation confirms optimal efficacy if intervention commences within early scar remodeling phase (3 months post-operation). Systematic craniosacral treatment can significantly improve tissue elasticity and tension distribution even for mature scars older than 5 years and relieve postural malalignment and associated chronic pain.
• Conclusion
Post-surgical postural deformity is not an inevitable surgical sequela, but systemic biomechanical imbalance triggered by occult scar adhesion along fascial-craniosacral axis. Understanding this mechanism urges clinicians to abandon partial treatment mindset and re-evaluate long-term surgical complications from integrated biomechanical and neurophysiological perspective.
As a safe non-pharmacological option, craniosacral therapy deserves further clinical research and popularization.
Glossary of core terms
1. Occult scar adhesion: Subcutaneous invisible fibrous adhesion formed in deep fascia, serosa or epidural space, the leading cause of chronic postoperative pain and postural abnormality.
2. Myofibroblast: Specialized cell with dual functions of extracellular matrix synthesis and smooth muscle contraction, primary effector cell of scar contracture.
3. Fascial continuum: Whole-body continuous connective tissue network governing biomechanical tension transmission.
4. Craniosacral system: Functional complex consisting of cranium, spine, sacrum, dura mater and cerebrospinal fluid, whose inherent rhythmic motion correlates closely with CNS function.
5. Cholinergic anti-inflammatory pathway: Neuroimmunomodulatory pathway whereby vagus nerve-derived acetylcholine suppresses excessive macrophage activation and pro-inflammatory cytokine secretion.